
Brief 19 is also available as an Adobe PDF file.
The West Virginia Medicaid program provides health care coverage to low-income adults and children and is one of the largest health care insurers in West Virginia. In fact, in 2003, an estimated 20% of West Virginians received health care services through the Medicaid program. Medicaid recipients are of particular interest to public health programs because many health conditions, including asthma, are inversely associated with socioeconomic indicators such as income. That is, individuals with low levels of income are more likely to have chronic health conditions. In fact, the prevalence of asthma is more than 2.5 times higher among West Virginia adults with an annual income less than $25,000 than among those with an income of $50,000 or more (14.1% vs. 5.4%)1.
1 These results do not include services provided under Medicaids managed care program. Approximately 16% of the Medicaid population was enrolled in the managed care program in the years 2001, 2002, and 2003.
West Virginia public health programs are working to reduce socioeconomic disparities related to chronic disease and access to health care. The first step is to identify and understand the burden of disease among West Virginians of low socioeconomic status. Therefore, the West Virginia Asthma Education and Prevention Program funded a project headed by Michael Smith, Ph.D., R.Ph., at the West Virginia University School of Pharmacy to analyze West Virginia Medicaid claims data to determine:
This brief compiles results of three separate analyses conducted by Michael Smith, Ph.D., R.Ph., at the West Virginia University School of Pharmacy. Presented are results from 2001, 2002, and 2003 West Virginia Medicaid fee-for-service claims data . Claims data are administrative data used for billing purposes. They provide information on all medical services and prescriptions billed to Medicaid for reimbursement. Disease conditions are identified by analyzing medical services diagnosis codes and prescription claims. Medicaid recipients were identified as having asthma if they had at least one medical service claim (office/clinic, ER, or hospital) with a primary or secondary diagnosis of asthma (ICD-9 CM codes 493.00-493.99), or at least two prescription claims for asthma-related drugs, of which at least one was for a drug other than an oral steroid. Oral steroids are used to treat many conditions other than asthma. Therefore, if a recipient had a claim for an oral steroid, he/she must also have had an asthma-related prescription claim for a medication in another pharmacotherapy class to be classified as having asthma.
The definition used to identify recipients with asthma is based on modified criteria of the National Committee for Quality Assurance (NCQA). It is important to note that this methodology may overestimate the prevalence of asthma, asthma-related medical service and prescription use, and asthma-related costs to Medicaid. Specifically, medical service claims with only a secondary diagnosis of asthma are included in the rates presented in this brief, although the primary reason for obtaining treatment may be unrelated to asthma. In addition, asthma-related prescriptions are used to treat other respiratory conditions, such as emphysema and bronchitis. Diagnoses are not identified in prescription claims; therefore, it is unknown for what specific condition recipients are being prescribed asthma-related medications.
We know that although there is currently no way to cure asthma, asthma symptoms can be adequately controlled through appropriate use of medication and avoidance of identified triggers. With proper management, individuals with asthma can live healthy, symptom-free lives. However, poor management of the disease can lead to complications resulting in hospitalization and even death. The purpose of this brief is to present one estimate of the burden of asthma among Medicaid recipients to inform public health professionals working to address asthma issues in this population.
Table 1.
Summary of Utilization of Asthma-related Health Care by West Virginia Medicaid Recipients
| TOTAL ASTHMA UTILIZATIONa | ||||
|---|---|---|---|---|
| Year | Number of recipients with asthma |
Prevalence rate per 1,000 recipients |
Total amount reimbursedd |
Average reimbursed per recipient |
| 2001 | 43,477 | 126 | $25,166,857 | $579 |
| 2002 | 42,312 | 119 | $28,304,831 | $669 |
| 2003 | 51,041 | 139 | $30,546,910 | $598 |
| MEDICAL VISIT UTILIZATIONb | ||||
| Type of utilization/Year | Number of visits | Rate of visits per 10,000 recipients |
Total amount reimbursed |
Average reimbursed per visit |
| Office/Clinic Visits | ||||
| 2001 | 33,226 | 965 | $3,305,622 | $99 |
| 2002 | 35,723 | 1002 | $3,431,757 | $96 |
| 2003 | 39,185 | 1068 | $3,837,147 | $98 |
| Emergency Room visits | ||||
| 2001 | 5,103 | 148 | $894,230 | $175 |
| 2002 | 5,642 | 158 | $1,007,981 | $179 |
| 2003 | 6,517 | 178 | $1,270,555 | $195 |
| Hospitalizations | ||||
| 2001 | 1,394 | 40 | $6,275,950 | $4,502 |
| 2002 | 1,702 | 48 | $7,941,660 | $4,666 |
| 2003 | 2,189 | 60 | $8,829,409 | $4,034 |
| PRESCRIPTION UTILIZATIONc | ||||
| Year | Number of claims for asthma-related drugs |
Average number of claims per recipient |
Total amount reimbursed |
Average reimbursed per recipient |
| 2001 | 141,108 | 8.5 | $6,499,946 | $393 |
| 2002 | 142,306 | 8.1 | $7,244,301 | $409 |
| 2003 | 137,420 | 8.1 | $7,021,517 | $414 |
| ASTHMA PREVALENCE |
|---|
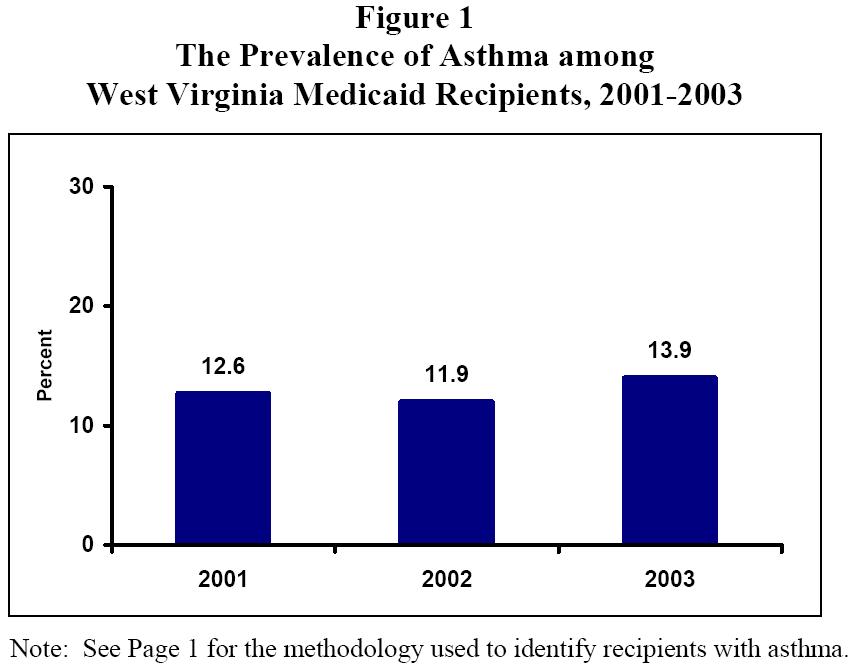
Between 2001 and 2003, the total number of Medicaid recipients increased from 344,296 to 366,987. In addition, the number of recipients with asthma2 increased from approximately 43,500 in 2001 to more than 51,000 in 2003. The percentage of Medicaid recipients who had asthma increased from 12.6% in 2001 to 13.9% in 2003.
In 2001, 2002, and 2003, the prevalence of asthma was higher among recipients that were aged 21 to 64 than those under the age of 15 and those aged 15 to 203. In addition, females were slightly more likely to have asthma than males, and the prevalence of asthma was more than 20% higher among whites than blacks. Between 2001 and 2003, the prevalence of asthma remained stable among most age, gender, and race groupings. Recipients 15 to 20 years old experienced the greatest increase in asthma prevalence, from 8.0% in 2001 to 11.1% in 2003.
2 Medicaid recipients were identified as having asthma if they had at least one medical service claim (office/clinic, ER, or hospital) with a primary or secondary diagnosis of asthma (ICD-9-CM codes 493.00-493.99), or at least two prescription claims for asthma-related drugs, of which at least one was for a drug other than an oral steroid. Oral steroids are used to treat many conditions other than asthma. Therefore, if a recipient had a claim for an oral steroid, he/she must also have had an asthma-related prescription claim for a drug in another pharmacotherapy class to be classified as having asthma. This definition is based on modified criteria of the National Committee for Quality Assurance (NCQA).
| ASTHMA-RELATED MEDICAL SERVICES USE |
|---|
Office/clinic visits are integral to proper asthma management. However, it is important to measure asthma-related acute care visits because ER visits and hospitalizations with a primary diagnosis of asthma are indicators of poor disease management and uncontrolled asthma.
Between 2001 and 2003, the rate of asthma-related hospitalizations increased 50% and the asthma-related ER visit rate increased 20.3%, whereas the rate of asthma-related office/clinic visits increased 10.9% (see Figure 2).
In 2001, 2002, and 2003, adults aged 21 to 64 and females had higher rates of all types of asthma-related medical service visits than other age and gender groups. The rate of asthma-related office/clinic visits was higher among whites than blacks, while blacks had higher rates of asthma-related ER visits and hospitalizations.
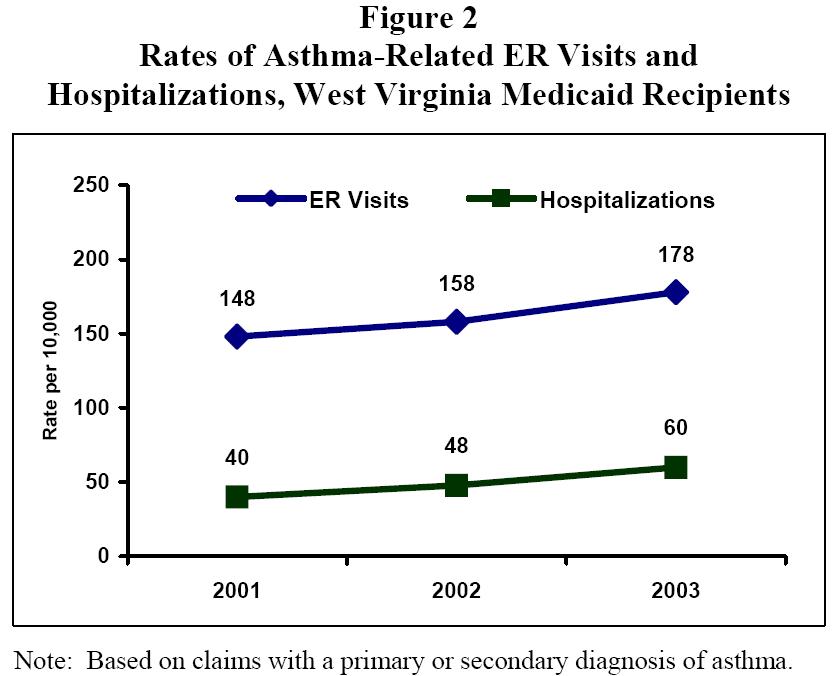
Note: Based on claims with a primary or secondary diagnosis of asthma.
| ASTHMA PRESCRIPTION MEDICATIONS |
|---|
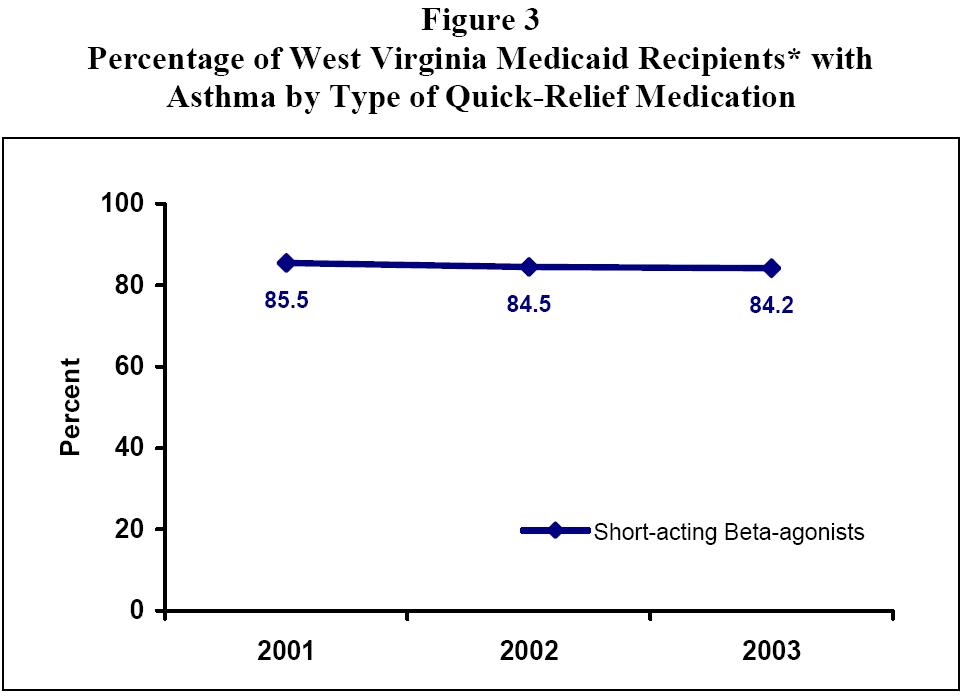
There are two main types of asthma medications. Quick-relief medications are used to relieve symptoms during an asthma attack. All patients with asthma should have access to a quick-relief medication. In the years 2001, 2002, and 2003, more than 8 out of 10 Medicaid recipients with asthma had filled a prescription for some type of short-acting beta-agonist, the most common class of quick-relief medication (see Figure 3).
Long-term controller medications are used to prevent attacks from occurring and are an essential component of a proper asthma management plan for patients with persistent asthma. Inhaled corticosteroids and leukotriene modifiers are considered first-line treatment medications for patients with persistent asthma. Between 2001 and 2003, there was an increase in the percentage of the total recipients with asthma who had a claim for a leukotriene modifier and a decrease in the percentage of total recipients with asthma who filled a prescription for an inhaled corticosteroid (see Figure 4). These results illustrate the percentage of total recipients with asthma who filled a prescription for a controller medication. Since asthma severity classifications are not recorded in claims data, it is unknown what percentage of patients with persistent asthma filled a prescription for a long-term controller medication.
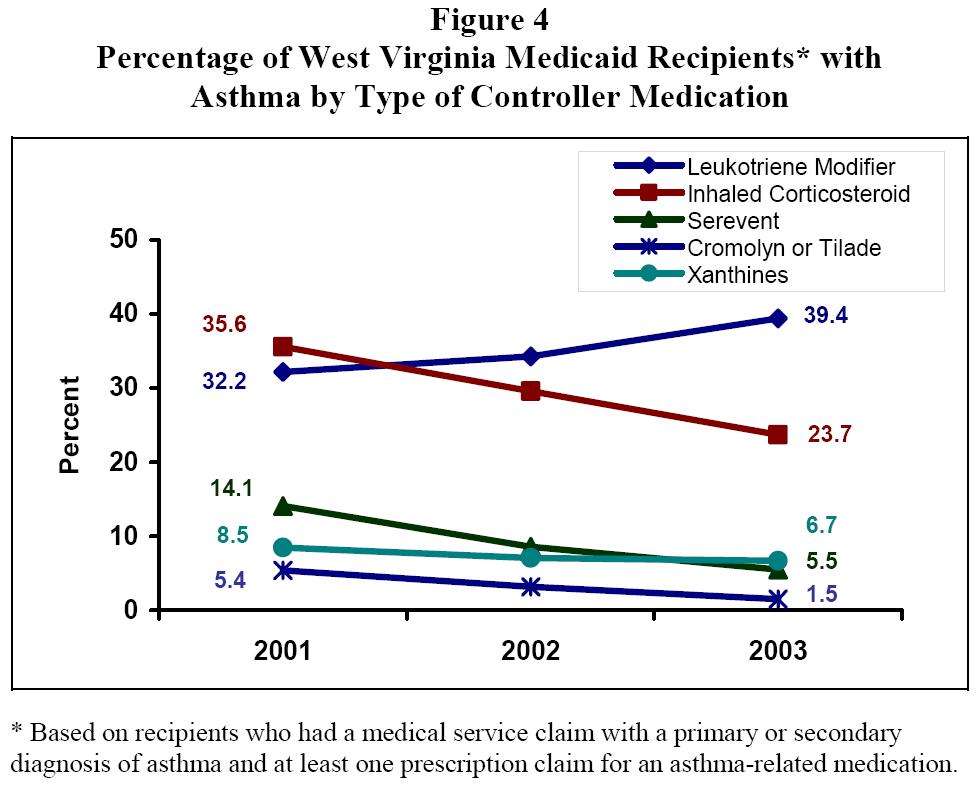
* Based on recipients who had a medical service claim with a primary or secondary
diagnosis of asthma and at least one prescription claim for an asthma-related medication.
| ASTHMA-RELATED MEDICAID REIMBURSEMENTS |
|---|
Between 2001 and 2003, there was an increase in the total amount reimbursed by Medicaid for asthma-related medical services and prescriptions. West Virginia Medicaid reimbursed $25.2 million for asthma-related claims in 2001, $28.3 million in 2002, and $30.5 million in 2003. This equals an average of $579 per recipient with asthma in 2001, $669 in 2002, and $598 in 2003.
Prescription medications and office/clinic visits accounted for 67% of the $30.5 million reimbursed by Medicaid for asthma-related claims in 2003 (see Figure 5). However, one-third of asthma-related reimbursements ($10.1 million) were for ER visits and hospitalizations, which are often preventable.
Hospitalizations are by far the most expensive medical service. In 2003, Medicaid reimbursed an average of $4,034 for every asthma-related hospitalization, compared with an average of $195 for every asthma-related ER visit, and an average of $98 for every asthma-related office/clinic visit.
A large portion of the increase in dollars reimbursed by Medicaid for asthma-related medical services is attributable to an increase in asthma-related hospitalizations (see Figure 6). Between 2001 and 2003, the number of asthma-related hospitalizations increased from 1,394 to 2,189 and the total amount reimbursed by Medicaid for these hospitalizations increased $2.5 million (from $6.3 million to $8.8 million). During the same time period, the total amount reimbursed for asthma-related ER and office/clinic visits combined increased by only $900,000.
It is important to note that these costs may be overestimated because they are based on claims with a primary or secondary diagnosis of asthma.
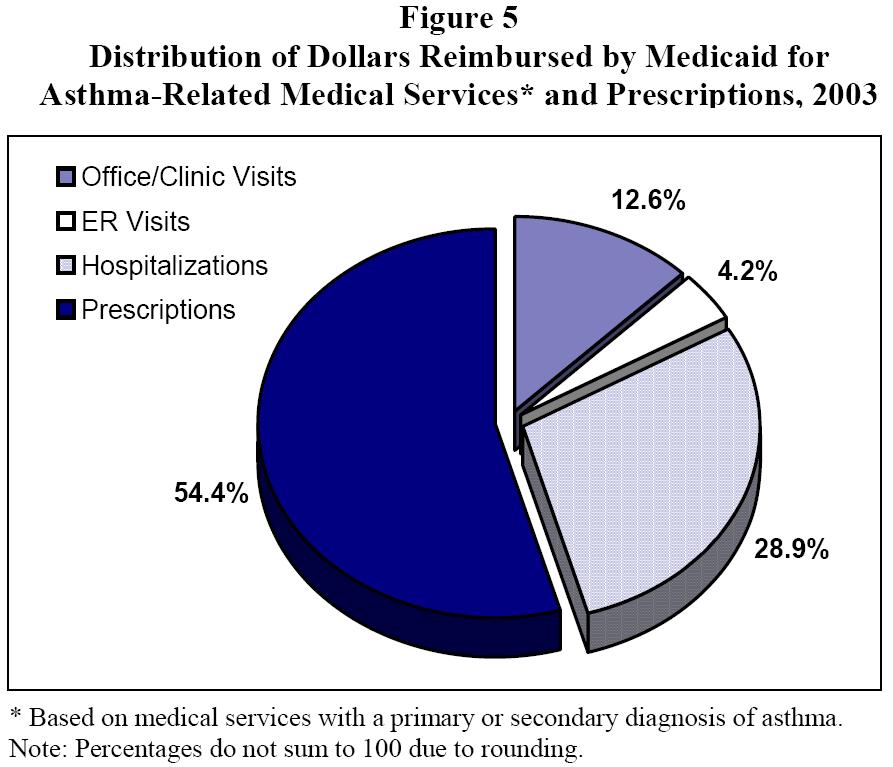
* Based on medical services with a primary or secondary diagnosis of asthma.
Note: Percentages do not sum to 100 due to rounding.
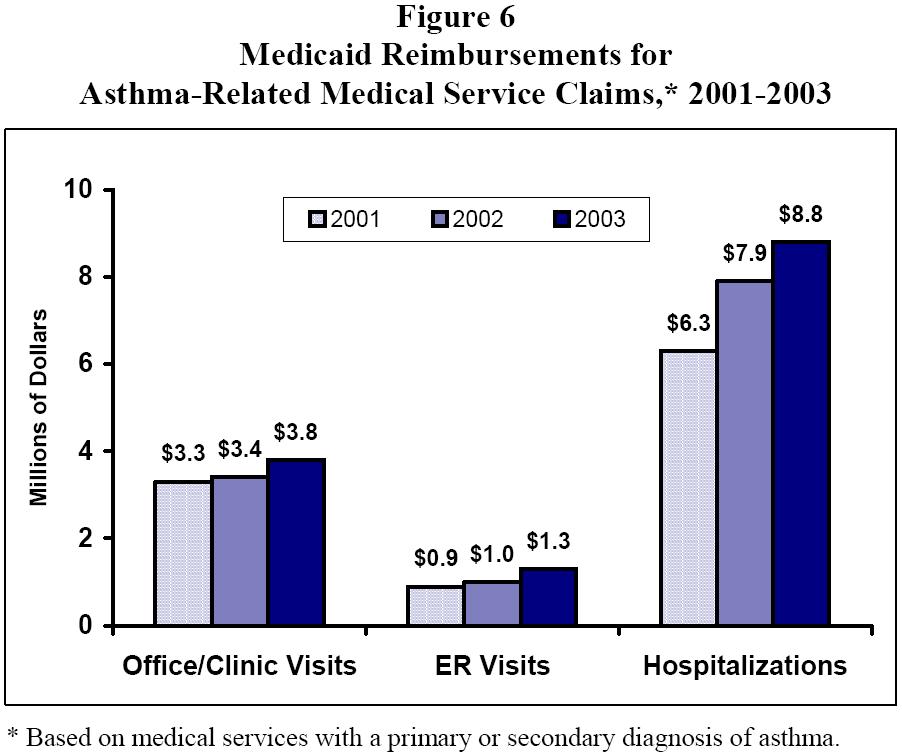
* Based on medical services with a primary or secondary diagnosis of asthma.
| CONCLUSION |
|---|
Approximately 1 in 5 West Virginians receive health care services through the West Virginia Medicaid Program and, according to the most recent estimates, nearly 14% of them have asthma. Asthma is a chronic lung disease that cannot be cured but can be adequately controlled through appropriate medication use and avoidance of identified triggers. With proper disease management, many asthma-related complications, ER visits, hospitalizations, and deaths can be prevented.
An analysis of 2001, 2002, and 2003 West Virginia Medicaid claims data indicate that the percentage of Medicaid recipients with asthma increased from 12.6% in 2001 to 13.9% in 2003. During this same time, the rate of asthma-related hospitalizations increased 50% and the asthma-related ER visit rate increased 20.3%, while the rate of asthma-related office/clinic visits increased 10.9%.
The amount of dollars reimbursed by Medicaid for asthma-related services increased by $5 million between 2001 and 2003 (from $25.2 million to $30.5 million). Although a majority of these dollars were reimbursed for asthma-related prescriptions, the amount reimbursed for asthma-related hospitalizations increased by nearly 40% (from $6.3 million in 2001 to $8.8 million in 2003). The total amount reimbursed by Medicaid for potentially preventable medical services visits (i.e., asthma-related ER visits and hospitalizations combined) increased from $7.1 million in 2001 to $10.1 million in 2003.
Further investigation is needed to better understand the burden of asthma among the West Virginia Medicaid population. It is unclear from these analyses why asthma-related ER visits and hospitalizations increased between 2001 and 2003. We do know that data from the West Virginia Health Care Authority indicate that there was an increase in the asthma hospitalization rate in the entire state between 2001 and 2003 (from 13.3 per 10,000 to 19.2 per 10,000) (2). However, additional research is needed to identify causal factors related to these increases in asthma-related acute care services among Medicaid recipients.
| REFERENCES |
|---|
|
West Virginia Health Statistics Center |
|
350 Capitol Street, Room 165 Charleston, WV 25301-3701 Phone: (304) 558-9100 Fax: (304) 558-1787 Web: http://www.wvdhhr.org/bph/oehp/hsc/default.htm |
|
| The Health Statistics Center (HSC) maintains West Virginia vital records and conducts the Behavioral Risk Factor Survey. The HSC can do customized reports and data analysis for grants, formal research, agency use, or specific community health planning activities. For additional information call the HSC and ask for a Statistical Services staff member. Visit the HSC website for electronic access to HSC reports and statistical briefs. This publication was supported by the Cooperative Agreement number U59/CCU324180-03 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention. It was produced in collaboration with the West Virginia Asthma Coalition. |
Last updated September 25, 2007.
If you have any questions, contact the Health Statistics Center at:
Phone: 304-558-9100 or
Email:dhhrvitalreg@wv.gov